Orthognathic Surgery
Everything you need to knowOrthognathic Surgery
Relocation and Shaping Surgeries for Jaw and Facial Bones
Asymmetries, developmental delays or overdevelopment anomalies in the skeletal structure of the face are common and may even create a structure specific to the region of residence. Changes that can be made to the bones in order to achieve facial proportions within an aesthetic understanding are evaluated within the scope of the sub-branch of plastic surgery called orthognathic surgery (maxillofacial surgery).
https://www.youtube.com/embed/73Bt8eY4WiQ?rel=0&autoplay=1&showinfo=0Maxillofacial surgery basically deals with the changes to be made in bone and soft tissue, and thus some definitions emerge. For example, occlusion basically means the correct contact of the teeth in the upper and lower jaw, while bite-related disorders are called malocclusion (wrong bite) . Malocclusion can significantly change facial expression. Although the overlapping of the right and left halves in the upper and lower jaw has been subjected to various classifications, the triple classification proposed by Angle according to the position of the first molars in the upper and lower jaw is the most frequently used. Accordingly, there are 3 main types of malocclusion. In the first one (Type I), although there is overlapping contact between the molars in the upper and lower jaw, the contact surface is inappropriate and the patient does not have developmental incompatibility in the upper and lower jaw. In the type called Type II, the lower jaw is further back than the upper jaw, while in Type III, the lower jaw is further forward and there are certain degrees of developmental delay in the upper jaw. Malocclusion may appear further forward on the lower and upper lips, in line with the more developed chin when viewed from the side.
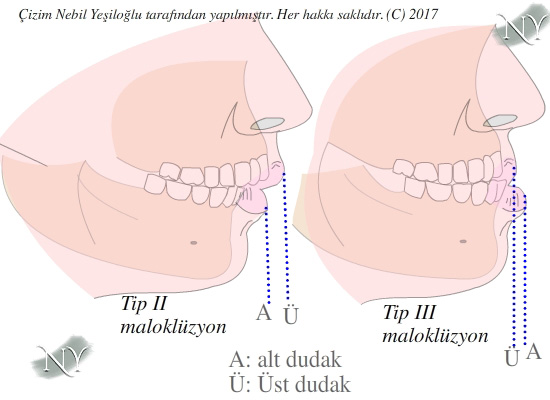
Image Note: Bad bite types according to Angle classification. Type I is described in the text.
Bite disorders are actually very diverse and can range from open bite deformity, where the patient's upper and lower jaw cannot close completely.

Image Note: Rear (A) and front (B) open bite problem.
Advancement and regression surgeries for the jaw and facial bones are performed while the patient is asleep, that is, under general anesthesia. Surgeries last between 2.5 and 4 hours. It can cause serious facial swelling.
Surgery planning is very important before orthognathic surgeries. Planning is done before orthodontic treatment and some changes may need to be made up to one day before the orthognathic surgery performed by the plastic surgeon.
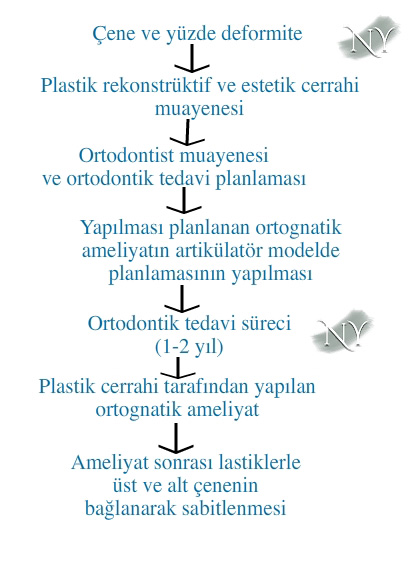
Image Note: Treatment steps in jaw surgery.
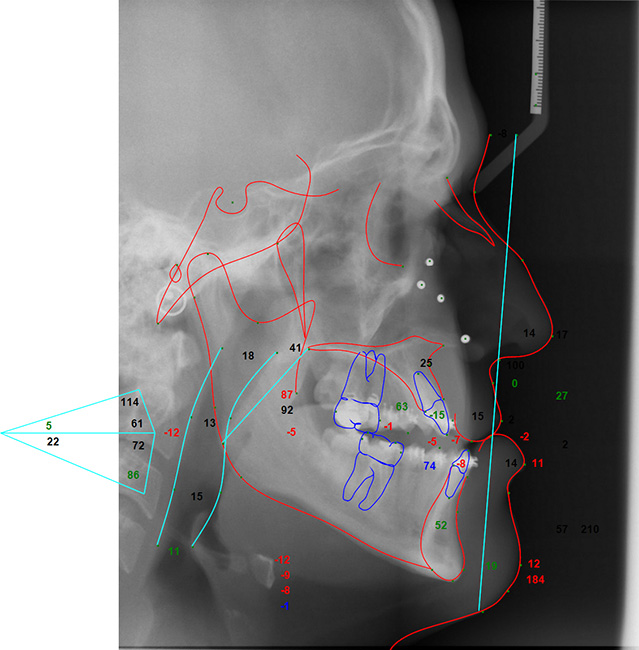
Basically, in this planning, a special x-ray study called cephalometric analysis is performed. In fact, on this planning, a simulation of the patient's surgery is applied and the reflection of the changes in the bone to the soft tissue after the surgery is evaluated.
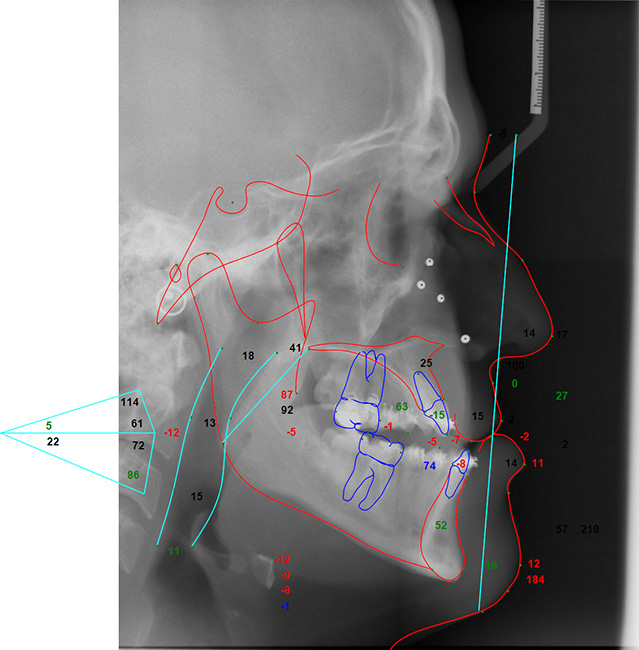
Image Note: Measurements of a Type III malocclusion patient with the lower jaw forward in the cephalometric analysis.
After planning, the patient is treated by the orthodontist and the orientation of the teeth is changed according to the surgery to be performed over a period of 6 months to 2 years.
Before starting orthodontic treatment, if the patient has an impacted tooth that would hinder the planned surgery, it will be removed by the plastic surgeon in a separate surgery session. When it comes time for orthognathic surgery, the plastic surgeon makes final evaluations based on the patient's cephalometric analysis. The day before the surgery, the orthodontist delivers two dental splints to the patient to be used during the surgery.
During the surgery, the bone structure is accessed through incisions made in the mouth and some incisions are made in the bones according to the planning. I prefer an ultrasonic cutter for these incisions. In this way, I observed that the patient's swelling was less and the patient healed faster.
After the bones are released, dental splints prepared by the orthodontist are placed and the lower and upper jaw are moved to the new position relative to each other. In this state, the bone is fixed with titanium plates and screws.
Surgeries to be performed on the upper jaw basically involve advancing the upper jaw bone, burying it towards the skull base (impaction), or pulling it down in the opposite direction of the skull base and rotating the upper jaw.
![Animation of Le Fort Type I upper jaw advancement surgery in a patient with developmental delay in the upper jaw. [All rights reserved (2016). Animation was made by Nebil YEŞİLOĞLU.]](https://www.drnebilyesiloglu.com/images/a/cene-yuz-ilerletme/cene-yuz-ilerletme-5.gif)
Image Note: Animation of Le Fort Type I upper jaw advancement surgery in a patient with developmental delay in the upper jaw. [All rights reserved (2016). Animation was made by Nebil YEŞİLOĞLU.]
These can be applied alone or together. In the lower jaw, advancing the jaw,
![Animation of lower jaw advancement surgery in a type II malocclusion patient. [All rights reserved (2016). Animation was made by Nebil YEŞİLOĞLU.]](https://www.drnebilyesiloglu.com/images/a/cene-yuz-ilerletme/cene-yuz-ilerletme-6.gif)
Image Note: Animation of lower jaw advancement surgery in a Type II malocclusion patient. [All rights reserved (2016). Animation was made by Nebil YEŞİLOĞLU.]
chin set back
![Animation of mandibular recession surgery in a type III malocclusion patient. [All rights reserved (2016). Animation was made by Nebil YEŞİLOĞLU.]](https://www.drnebilyesiloglu.com/images/a/cene-yuz-ilerletme/cene-yuz-ilerletme-7.gif)
Image Note: Animation of mandibular recession surgery in a type III malocclusion patient. [All rights reserved (2016). Animation was made by Nebil YEŞİLOĞLU.]
There are also surgeries that involve turning the jaw to the right or left in different axes.
If the amount of advancement in the bone will be over 10 millimeters, the patient should be treated by establishing a gradual advancement system called distraction. Otherwise, the patient's problem may recur. For detailed information about distraction, please follow the future articles on my blog.
On the first day after the surgery, a rubber band will be applied to your previously placed braces for fixation, and the duration of this is approximately 20-30 days. During this period, you need to eat liquid foods. Your hospital stay is 2 or 3 days.
The shapes of bone incisions in the upper jaw were defined as different types by French surgeon Rene Le Fort, and these are related to the type and degree of facial deformity.
Surgeries that change the location of facial bones are not limited to the upper jaw and lower jaw. Many forms of surgery have been described for many facial deformities. (You can get detailed information about these from your doctor.) For example, Le Fort osteotomies defined for the upper jaw and upper face area are of three types and involve the mobilization and advancement of the facial bones from various points.
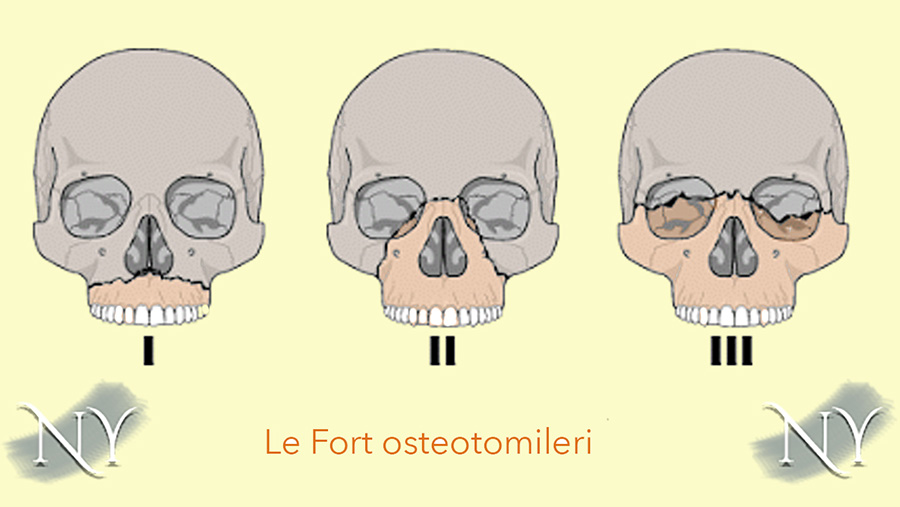
Image Note: Types of upper jaw and upper face advancement surgery according to Le Fort.
In some patients, these are not sufficient and full facial advancement, called monoblock advancement, may also be necessary.
Not everyone may be a suitable candidate for surgery that reshapes the jaw and facial bones by changing their length. Although this surgery seems theoretically possible to anyone, it is especially suitable for people under the age of 35. I discuss with you the feasibility of this surgery by evaluating all the necessary conditions in your application.
Orthognathic surgeries are long-lasting and can tire the patient. Therefore, it is preferred that the patient does not have internal or metabolic diseases (such as diabetes, uncontrolled hypertension, heart, liver or kidney failure), is under 30 years of age and is a non-smoker if possible.
One of the most basic conditions required for orthognathic surgery is that the patient has sufficient bone density. The plates and screws placed in patients with osteoporosis will not fit securely, and the bone incisions will heal very slowly. The likelihood of recurrence of malocclusion is also higher in these patients.
Lower and upper jaw advancement-retraction surgeries are not completely problem-free. It is possible to easily solve these problems in cooperation with your surgeon. Some may require readmission to the operating room.
Problems that may be seen after orthognathic surgery are:
1. Blood accumulation (hematoma) under the incision line, infection; It is a problem that can be seen after every surgery. The hematoma may need to be drained and the bleeding stopped if there is a focus. In the presence of infection, hospital follow-up and treatment may be required.
2. Recurrence of the problem (relapse, recurrence); The likelihood of the problem recurring increases, especially in the lower jaw that is advanced more than 10 mm. This condition may require corrective surgery.
3. Lower lip numbness; It occurs due to damage to the mental nerve running in the lower jaw bone during bone incision and advancement in the lower jaw and may be permanent.
4. Bone nonunion problem; It may occur more frequently in patients with low bone density. The presence of an impacted tooth, especially one that has not been extracted, in the bone incision line may constitute another reason and may require re-operation.
5.Mandibular joint dislocation; It may occur in patients whose lower jaw bone is advanced. If proper fixation is not made on the bone parts, re-screwing may be required in the operating room.
6. Deformity of the nose; When the upper jaw is advanced, the nose may also move forward and upward above a certain level. This situation will already show itself in preoperative simulations and may require corrective rhinoplasty, that is, nose plastic surgery.
Alternative surgery options are also available for patients whose lower or upper jaw is lagging and whose development is delayed. These can sometimes be applied together in displacement surgeries in the lower and upper jaw bones.
Surgeries to shape facial bones can be limited to patients with mild to moderate developmental problems and can be corrected with artificial implants (prostheses). Although many implant derivatives have been developed today, porous polymethyl methacrylate (PMA), porous polyethylene or silicone implants are often preferred in the facial area. While the first two of these are fixed to the bone with titanium screws, some brands have holes for silicone to be fixed with stitches. Silicone type facial implants are likely to slip from their location and should be replaced approximately every 10 years. In other implants with a porous (perforated) structure, soft tissue and vessels multiply over time through the microscopic holes of the implant and surround the implant, so slipping of the implant is not expected.
Genioplasty is a surgery performed to shape the tip of the lower jaw and is performed either by making incisions in the bone or by using artificial implants.
Although patients generally present with bite problems in orthognathic surgery, a small number of patients either do not have any problems or can be largely resolved with orthodontic treatment. In these patients, a surgery called genioplasty can be performed to clarify the tip of the chin if the lower jaw is left behind. After the gel-like hyaluronic acid fillers or the fat taken from the body are injected, they will melt over time, resulting in a decrease in the volume of the chin tip.
Genioplasty is performed with the person's own bone tissue (osseous genioplasty) or with artificial implants. In osseous genioplasty, a bone incision is made at the tip of the lower jaw according to cephalometric measurements, movement is provided in various directions such as forward, backward, up, down, right, left or a combination of these and fixed with titanium plates and screws.
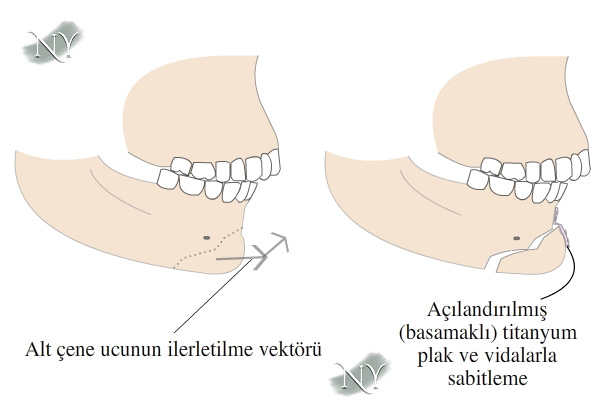
Image Note: Shaping the tip of the jaw with an incision made at the tip of the lower jaw bone, that is, osseous genioplasty.
In genioplasty performed with implants, if hard porous implants are used, they are fixed with titanium screws, while those with silicone base either fit into the pocket on their own or are fixed at special points with stitches.
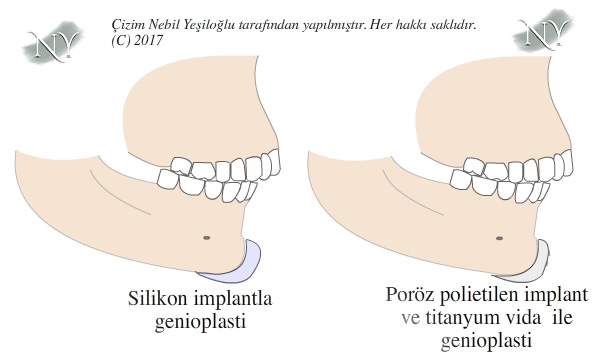
Image Note: Genioplasty with implants.
Silicone implants have the possibility of slipping.
Genioplasty surgery is performed through intraoral incisions, takes approximately 1.5 hours and will leave no visible scars from the outside.
In the evaluation before genioplasty, whether the patient has sagging or fat accumulation, especially in the jowl area, may indicate the need for intervention in this area. In this case, genioplasty combined with liposuction is applied.
The use of zygomatic and cheek plumping implants may be necessary, especially in patients whose eyeball is positioned more anteriorly than the cheekbone (negative vector condition).
In eyelid aesthetic surgeries, especially when intervening on the lower eyelid, it may be possible to place a permanent implant for the cheek in patients with a receding cheekbone. Thus, the aesthetic result obtained may be more satisfactory. Polyethylene or polymethyl methacrylate-based polymeric and perforated implants are often used for this type of plumping. These also integrate well with soft tissue. Very rarely, these implants may be seen as a foreign object by the body in the long term and may be discarded. In such a case, they may cause abscesses in the area. Implants must be removed from the surgical field that has become like this.
Another requirement for removal of cheek implants is implant breakage. Fractures may occur in solid implants due to blows to the face. In this case, the implant may need to be replaced.
Cheek implants can be placed in two separate areas. One of these is an under-eye incision on the lower eyelid, while the other is inside the mouth. In the second, the incision scar is not noticeable from the outside. Implants are fixed to the bone with titanium screws. Surgery time is approximately 1 hour. Fat injection may be applied to the area.
"Health is the most important thing you have in life!"
Contact us now to schedule an appointment.