Facial and Jawbone Repairs
Everything you need to knowFacial and Jawbone Repairs
The nasal bone is the most frequently broken bone due to its protruding structure on the face. Most nasal fractures can be replaced with a closed technique.
One of the main issues of plastic surgery is the elimination of fractures in the facial bones and deficiencies in these bones due to impact or cancer surgery. The bones that make up the face consist of the forehead bone (frontal) on the upper face, the nasal bone, cheekbone (zygoma) and upper jaw bone (maxilla) on the middle face, and the lower jaw bone on the lower face.
The nasal bone is the most frequently broken bone due to its protruding structure on the face. Most nasal fractures can be replaced with a closed technique.
The nasal bone, which forms the midpoint of the face, can be damaged alone or together with the nasal cartilages that form its continuity when broken.

Visual Note: Advanced deformity and x-ray image of nasal fracture
When there are fractures in other facial bones, they are often accompanied by nasal fractures. After the impact, the nasal bone may break in one or multiple pieces. Settlement of the fracture is done with regional anesthesia (nerve block). With a tool placed inside the nose, the nasal bone is supported from below. After the intervention, a nasal splint is placed on the nose. This splint is removed after 1 week. A possible problem after nasal fractures is blood accumulation (hematoma) in the septum, the middle compartment of the nose. Septum hematoma should be drained by making a small incision in the nose while the fracture is seated. Very rarely, there may be bleeding in nasal fractures that does not stop despite the application of tampons, and these may require endoscopic examination and cauterization. Because the bleeding focus left in place may cause melting in the septum after a while, causing holes to appear. After the nasal fracture is set, nasal plastic surgery may be required to correct the edema and correct it again.
Lower jaw bone (mandible) fractures, like nasal fractures, are common and may require surgical treatment. As a result of these treatments, changes in tooth alignment may occur and these may need to be corrected with orthodontic treatment.
The mandible, that is, the lower jaw bone, which is one of the protruding bones of the face like the nose, can often be broken due to fist blows. Generally, a blow received from one side causes a fracture in the bone both at the point where the blow was received and at the point that bears the pressure on the opposite side of the blow. Fractures between the fracture ends that distort the shape of the face and prevent the teeth from sitting properly in the biting position may require surgical treatment. Mandibular fractures are often observed in the neck region and body (corpus) of the bone, called the subcondyle.
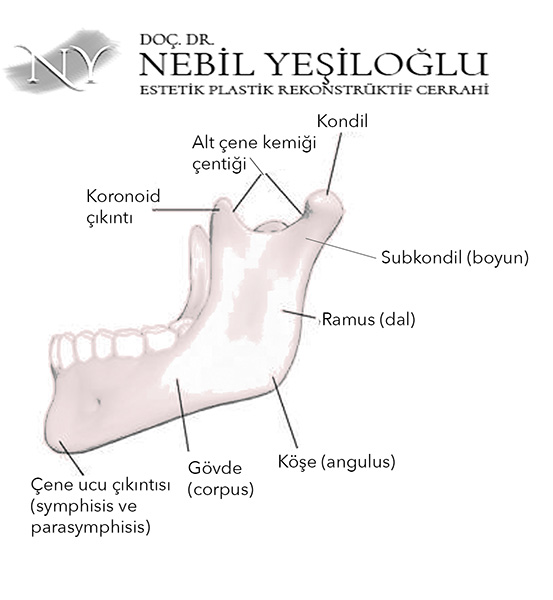
Image Note: Parts of the lower jaw bone (mandible)
In fractures involving only the neck area, if there is no serious angulation, union can be observed with closed monitoring for a while.
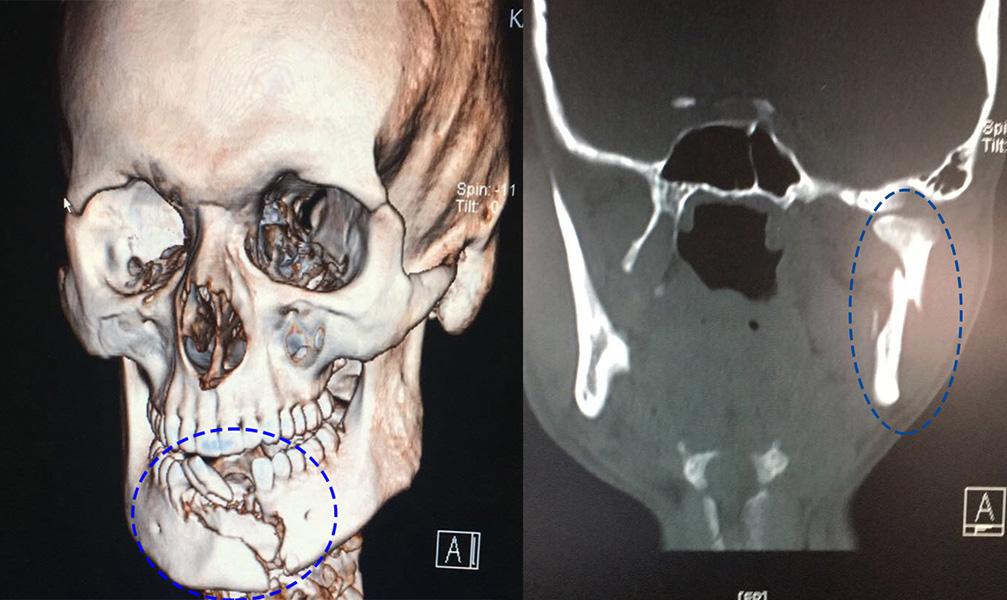
Image Note: Fracture occurred in the lower jawbone at the tip, in the parasymphysis region (left) and in the subcondyle region (right).
During this period, an elastic bandage can be applied, or in patients who have problems with teeth overlapping, braces can be worn and the upper and lower jaws can be connected to each other with elastics. A plastic surgeon will make the necessary comments on this matter.
In lower jaw fractures, if there is no injury to the skin close to the fracture, the fracture is repaired with intraoral incisions. During the surgery, the fracture ends are cleaned and repaired with titanium plates and screws. It is recommended to remove these plates and screws with a second surgery after 3-4 years. Dissolvable plates can also be used in repairs on babies and young children. I do not prefer these in adults because their resistance is not like titanium.
After mandibular fracture surgery, it is recommended to drink liquid food for a period of time deemed necessary by your doctor depending on the location of your fracture.
The zygomatic bone is one of the protruding areas on the lateral side of the midface and participates in the formation of the ogee line, which is the basic aesthetic line of the face in diagonal view [for ogee lines, please see the facial aesthetics section].
In the mid-face region, the zygomatic bone, at the level of the nose, articulates with other bones through four separate protrusions. For this reason, blows that displace the cheekbone often affect other bones as well. The horizontal protrusion of the zygomatic bone is called the arch, and the coronoid protrusion of the lower jawbone enters and exits the immediate inner side of the arch when the mouth is opened and closed. There may be difficulties in opening and closing the mouth in bow fractures. In this case, the zygoma spring is inserted into place through an incision made in the scalp.
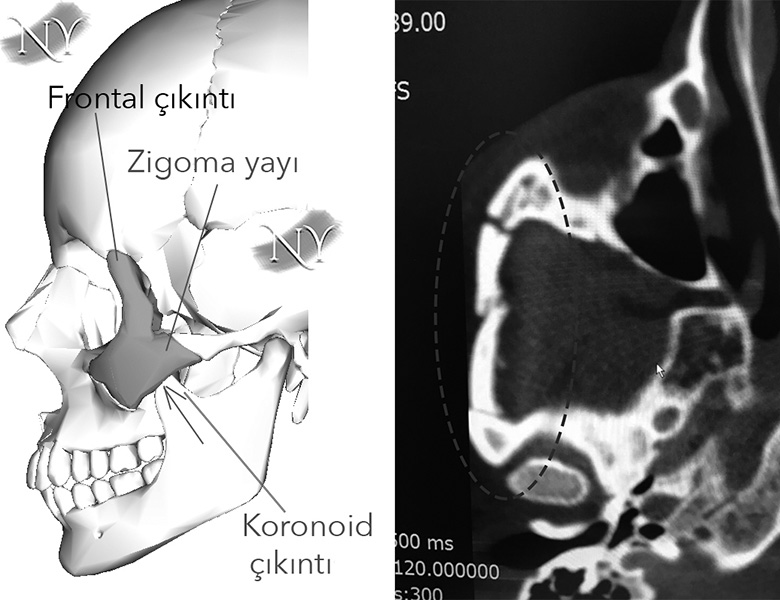
Image Note: Position of the zygomatic bone on the face (left) and fracture of the zygomatic arch (right).
This surgery takes approximately 5 minutes. It can also be done with regional anesthesia. If the spring collapses again in resistant cases despite this correction, open surgery and fixation with plates and screws may be required.
In zygomatic bone fractures, the connection of the fracture with neighboring structures is important. These connections will affect the treatment to be given.
The upper jaw (maxilla) bone is the basic element that connects the lower face to the upper face, and its fractures can cause serious facial deformities and speech disorders due to air leaks in the pharynx area. Therefore it should be handled carefully.
Upper jaw bone fractures often occur with high-energy impacts such as falls from a height and traffic accidents. It is more common with other bones of the face. The main factor determining the treatment for upper jaw fractures is the type of fracture. Maxilla fractures were classified into three main types, from mild to severe, by French surgeon Rene Le Fort.
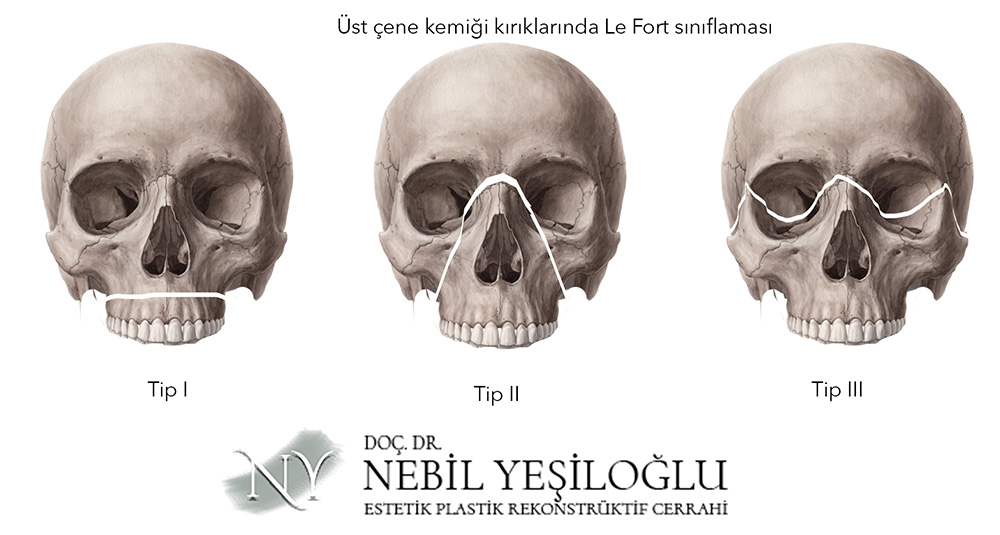
Image Note: Le Fort classification in upper jaw (maxilla) fractures.
In the first type, the lower part of the upper jaw bone, called the dental arch, is separated from the skull base and this type of fracture can be treated with an intraoral approach. In the second and third types, the fracture also includes the eye socket and surgery is performed by entering through an incision line made through the scalp. These fractures often do not occur alone.
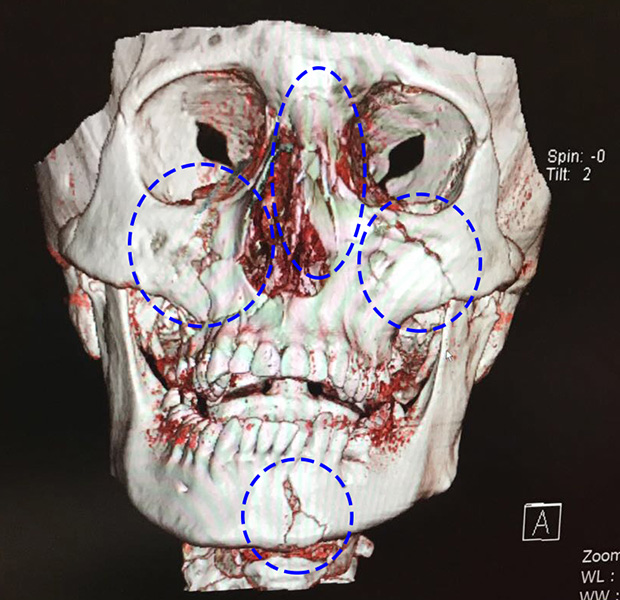
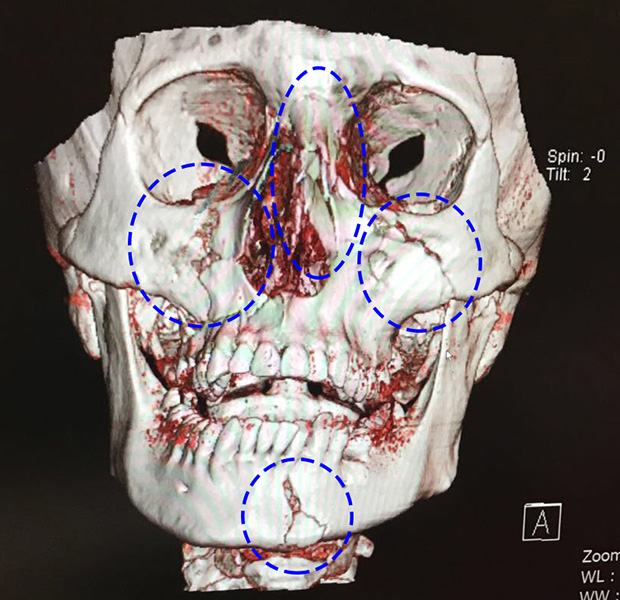
Image Note: Three-dimensional tomography of the combined fracture of the nose, zygomatic and upper jaw bones and lower jaw on the face.
In fact, in some patients, different types of fractures occur on both sides.
The main treatment for upper jaw fractures is surgery in which the bone is fixed with titanium plates and screws. In rare cases, it can be continued with follow-up in the patient who does not have a bone shift.
The eye socket (orbita) is formed by the protrusions of 7 bones and is like a cube that narrows towards the back. It is observed that it is frequently affected by facial fractures.
Every blow to the eye is reflected into the eye socket (orbita) by the mass effect of the eyeball. The thinnest and weakest of the walls on which the impact is reflected is the floor of the eye socket, where the bone becomes as thin as a leaf. Due to the impact, the eyeball tends to slide into the sinus cavity below, causing a fracture in the weak orbital floor bone. The eyeball, surrounding eye muscles and underlying fatty tissues protrude beyond the orbital boundaries and are defined as blow-out fractures.
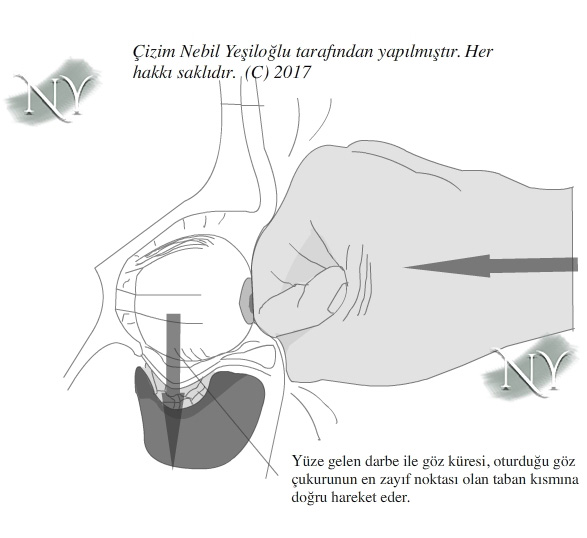
Image Note: In blow-out fractures of the orbit, it is common for all soft tissues in the orbit to slide downwards.
In these fractures, the muscles that move the eyeball may get stuck in the fracture line, and in this case, strabismus and double vision may occur. It is recommended that these patients be evaluated quickly and operated on as soon as possible. Because the blood supply to the muscles may be impaired at the compression line and may become permanently dysfunctional. Eye muscles can also be directly injured in eruption fractures. In this case, different surgical solutions may be recommended to prevent strabismus and double vision.
If the person has conditions such as displacement of the eyeball, strabismus, double vision, severe deformity due to fractures of other walls of the eye socket, the patient should be operated on.
After surgery for facial bone fractures, the patient's own care is also important. Ask your doctor for detailed information on this subject.
Surgical treatment of facial fractures takes from 5 minutes to 3 hours depending on the degree of location of the fracture, and if there are bone deficiencies or dead bone tissues, repair may be required with a bone patch or artificial materials taken from another part of the body. In these surgeries, incision lines that are not visible from the outside, such as inside the mouth or inside the scalp, are used whenever possible.
Facial fractures often occur in combinations rather than singly. Therefore, possible risks should be explained to the patient during surgery planning.
After facial fracture surgeries, the patient's bed should be bent up from the waist and ice application is recommended for 10-15 minutes per hour. Ice application will allow edema and swelling to resolve faster.
Your incision lines will heal within 7-14 days. The stitches of intraoral incisions are expected to dissolve on their own. Skin stitches are removed at the end of the healing period. Your bruising and swelling will disappear within 15-20 days.
In the treatment of facial bone deficiencies, bone patches taken from various parts of the body can be used, as well as artificial implants that mimic bone.
In order to create the aesthetic units of the face in plastic surgery, the skeleton needs to be supported in some patients. Our main sources for bone tissues that can be used for this purpose are the pelvis, the fibula bone in the leg area, the outer layer of the skull bone, bone ribs, the elbow protrusion or the protrusion on the front surface of the shin bone (tibia) in the leg (tuberositas). Since bone patches longer than 4-5 cm may have feeding problems in the bed where they are transferred, it is necessary to take the bone patch together with the vein from which it is fed, whenever possible. This is called a bone flap . Surgeries using bone flap take approximately 2-4 hours. The vessels of the bone are connected to the vessels in the recipient area using a microsurgical method.
Apart from bone, artificial implants, especially porous polyethylene or polymeric methacrylate derivatives, can also be attached to the missing area of bone with screws or stitches. Although these artificial products are tissue compatible, there are also patients who perceive them as foreign substances in the long term and remove them after causing discharge and infection. Artificial materials are advantageous because they do not require taking tissue from elsewhere in the body and are placed in a shorter time.
Titanium and polymer materials used in the repair of facial fractures are all compatible with magnetic resonance imaging (MRI).
"Health is the most important thing you have in life!"
Contact us now to schedule an appointment.