Ear Aesthetics
Everything you need to knowEar Aesthetics
Ear Aesthetics - The main problems seen in the newborn baby are the prominent (sail) ear, faint or very obvious ear recesses and protrusions, the earlobe being too forward and prominent, partial (microtia) or complete absence of the ear along with the ear canal. (anotia) are deformities such as cup ear, telephone ear, pointed ear (Spock ear) due to deformities of the ear folds.
Our ears actually consist not only of a roughly funnel-shaped structure called the ear canal or pinna , which allows sounds to reach the middle ear in waves, but also of hearing structures called the external auditory canal, eardrum and ear ossicles, and a balance organ called the cochlea. However, the area of interest of plastic surgery is the auricle, and on this page we will consider the concept of ear only as the auricle.
The expected upper limit of the ear is generally at the level of the top of the eyebrows. The position of the lower border changes depending on its length. While the angle of the ear with the skull is approximately 30 degrees, the distance to the skull is around 20 mm. Above these values is considered a frequently seen prominent ear deformity.

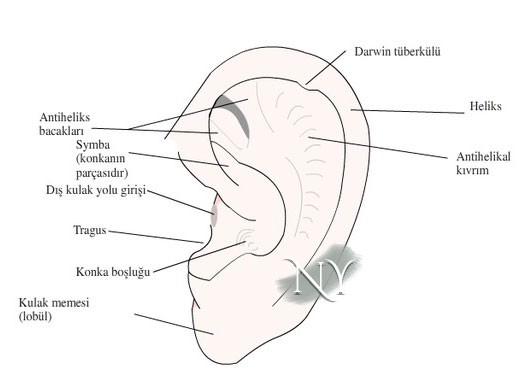
Image note: Anatomical structures of the ear canopy.
When aesthetic problems of the ear are observed in the newborn baby, they can be reversed in the first 2 weeks with the use of special molds and bandages called splinting.
The main problems seen in the ear in a newborn baby are: prominent (sail) ear, indistinct or very prominent ear recesses and protrusions, earlobe being too forward and prominent, partial (microtia) or complete absence (anotia) of the ear along with the ear canal. These are deformities such as cup ear, telephone ear, pointed ear (Spock ear) due to deformities of the ear folds. Since prominent ears are frequently seen, I have only included prominent ear deformity on this page in order to avoid creating information pollution. Other problems are actually the subject of reconstruction surgery and you can follow the upcoming articles on our blog page.
In newborn babies, where the ear is only deformed but its structures are not missing, the shape change can be achieved by making some kind of splinting using molds and special bandages placed in the ear folds in the first weeks, since the cartilage is loose due to the effect of estrogens passed from the mother. However, in such splints, the ear should be checked regularly to prevent pressure-related wounds.
Contrary to popular belief, thread ear aesthetics may not be a suitable solution for patients who are rigid and do not bend easily. Due to cartilage memory, frequent re-openings are expected.
I often get asked from my patients whether I do ear surgery with thread. I perform this mini-surgery by explaining the high probability of re-openings after the intervention in a limited number of my patients who insistently request non-surgical ear aesthetics. I say mini-surgery because in practice, it is necessary not only to fold the ear by passing subcutaneous stitches behind the ear, but also to weaken the resistant ear folds by making cuts from the inside, and in fact, all of this should be considered as a surgery. The duration of the intervention is approximately half an hour for both ears, and then I recommend the use of terry bandages used by athletes for at least 2 weeks. Postoperative dilatation can also be observed in the early period. In such a case, it is necessary to either switch to open surgery or repeat the intervention with new threads.
Protruding ear surgery can also be performed without putting the patient to sleep. General anesthesia is the most ideal method for our younger patients.
Protruding ear surgeries are performed through incisions behind the ear and include resistance-reducing incisions or rasping, and bending maneuvers with permanent stitches in shadows where the angulation of the ear cartilage is insufficient. In patients with forward earlobes, special stitches should be placed for this structure. Finally, the ear skin is closed with stitches that dissolve by the body in approximately two weeks, and a special ear dressing is applied.
The surgery can also be performed on a patient patient after the age of 16, using regional anesthesia without anesthesia. However, in terms of patient comfort, the ideal thing is to put the patient to sleep. The auricular block performed at the end of the surgery ensures that the first hours after the surgery are pain-free. After the effect of this block wears off, treatment with painkillers is continued.
For patients who think their ears are too large, a comparison roughly called the ear-to-nose ratio may be useful. I tell my patients whose ears are large that there may be visible scars from the incisions made for reduction.
If you think your ear is larger than normal, you can roughly compare the distance between the nose root and nose tip with the length of the ear from top to bottom. In fact, these lengths are quite close to each other. In cases where your ear length is obviously longer, reduction can be made with techniques that cause visible scars in the front part of the ear. The average ear length is 6-8 cm and its width is around 1.5 cm.
I recommend athletes use towel bandages for about 15 days after prominent ear surgery. Patients can take a shower at the end of the second day.
After prominent ear surgery, I recommend that my patients, especially those who undergo surgery under general anesthesia, stay in the hospital for one night. This allows any pain that may occur to be easily controlled with intravenous medications. There may be pain for up to 3-4 days on average. If the pain becomes increasingly severe, problems such as tension due to blood accumulation behind the ear or infection in the ear cartilage may be considered. Therefore, inform your doctor as quickly as possible. Generally, these two problems I mentioned are solved with early treatment before they get worse. In some patients, especially in those in whom we perform ear cartilage abrasion, swelling and redness in the auricle may occur during the first week. These swellings, which are usually asymmetrical, regress with some edema-resolving treatments. Regular use of the bandage is also important in this sense.
On the second day after the surgery, I remove the ear dressings of my patients and after a short cleaning, I place some wick-shaped cotton behind the ear. The patient changes this cotton pad after every shower and daily and applies a prescribed pomade to the area after leaving the hospital.
Re-openings may be observed after plastic surgery of the ear. The frequency of this occurring varies depending on the patient's care and surgical technique.
Common postoperative problems in ear aesthetics are problems such as results being below expectations, edema and swelling, infection in the wound line, blood accumulation under the incision (hematoma), cartilage stitches becoming visible from the outside, earlobe problems, telephone ear deformity. In the late period, re-increases in ear opening (recurrence of prominent ears) may also occur. These problems are basically related to surgical technique and patient care, and it is possible to re-treat. Infection at the wound line and subcutaneous blood collection, although rare, may require readmission to the hospital and intervention in the operating room. Thanks to the drain placed in the incision line at the end of the surgery, I do not encounter any problems with blood collection. This drain is removed the morning after the surgery.
Telephone ear deformity is based on the fact that these two extreme parts remain more prominent in patients who generally receive more correction at the middle point of the ear than the upper and lower poles. Requires correction in the operating room.
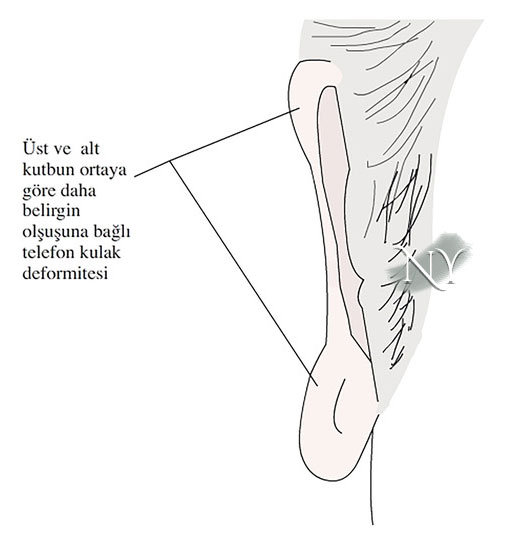
Visual note: Telephone ear deformity due to overcorrection of the middle level of the ear or undercorrection of the earlobe or upper pole.
Earlobe correction is one of the most important and most difficult parts of prominent ear surgery.
If there is a highly forward earlobe before surgery due to the possibility of it opening forward again, stitching and tissue advancement techniques should be used to move the earlobe back. Some of these techniques involve gluing the earlobe to the adjacent skull area. Such techniques are not suitable for girls due to the possibility of wearing earrings.
"Health is the most important thing you have in life!"
Contact us now to schedule an appointment.